DNA Fraud
- johnbutton2
- Feb 24
- 5 min read

Continue the Macartney case
To obtain a full DNA profile, one molecule is taken from a single cell and tested at 10 points (loci). For each locus, 2 numbers are given. Since each of your parents has 2 numbers, you inherit 1 from each, giving you a unique profile.
When Senior Scientist Lawrence Webb produced Lalita’s DNA profile in court, he was asked by the defence lawyer, “What does the REF stand for after her name?”

His reply was “Because we were unable to get a DNA profile from her body, it has been referred from another Item in evidence.” (They could not even determine her sex from the AMEL Loci)
It appears that from a possible 20 numbers on her body and 200 from all of her 10 fingernails, they could only manage 4 numbers and an X/X.
THEN WHY NOT TAKE MORE SAMPLES?
This is where it gets ugly and deceitful.
May I be permitted to logically draw conclusions?
On Tuesday evening, 5 December 1999, Dr Cooke, Pathologist had Lalita’s body sent from the place of her death to Perth.
The earliest the family could have met with the undertaker is Friday, 10 December. (The PM was concluded late Thursday night)
The Cremation was carried out on Tuesday, 14 December. Without a cause of death being established.
I wrote to the coroner and asked if it was common to cremate a body so soon after the PM and without time for a defence lawyer to consider if he needed any more tests done to establish the cause of death.
His reply
However, in many instances, it wont be obvious to the pathologist at the Post Mortem examination and as such they may request further testing of bloods, urine, tissue, etc. In these instances, the pathologist will write “UNDETERMINED (PENDING INVESTIGATION)”. The “Pending Investigation” part is where they await the results of toxicology and/or other testing.
Upon the additional results being provided to the pathologist, they will either be in a position to identify/stipulate a definitive cause of death, or they will write “Unascertainable” or as you have stipulated “UNASCERTAINABLE (CONSISTENT WITH APHIXATION)”, as some times notwithstanding all of the testing and examination performed, the pathologist is simply not able to provide a definitive cause. Also, as you have indicated, sometimes they pathologist can’t be definitive, but they will indicate consistent with xxxxx.
So in answer to your final question, “should the permit have been issued when the coroner knew that the testing for cause of death had not been done yet?”, yes that is standard practice because all of the testing would have been done at the PM examination allowing the body to be released, and there is no need to hold the body until the final PM report is provided.
So what is the coroner really saying here?
Yes, it is standard practice for the body to be cremated before the testing has been done.
Or, I permitted the body to be cremated because it is standard practice for ALL testing to be done before the PM report is sent to me.
Had all testing been done?

Geraldton Cemetery Board
Yes I can help you with that information.
Lalita passed on the 5/12/1999 and was cremated on the 14/12/1999.
Thankyou
Casey Campbell
Administrator
130 Eastward Road, Geraldton WA 6530
Date of Laboratory tests
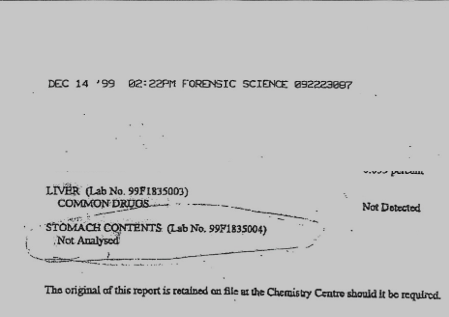
The stomach contents had not been analysed before she was cremated. WHY NOT? Were they told not to?
The pathologist told the court he had not performed any tests. This is his reason:
“Well, there are some grains of truth in what you say, but now we know that asphyxiation does not always produce those signs.”
These are the signs he should have been looking for
1. Petechial haemorrhages: Tiny red or purple spots caused by burst capillaries, commonly found on the face, eyelids, and conjunctiva (the whites of the eyes). Additionally, on mucosal surfaces (such as inside the lips and gums). There had always been some external indication as well.
2. Cyanosis: a bluish discolouration of the lips, fingertips, or extremities due to lack of oxygen.
3. Pressure marks or ligature marks: If duct tape or any form of binding was used, there should be marks on the neck or mouth where pressure was applied.
4. Blood in the nose or mouth: occasionally seen if forceful suffocation caused trauma or pressure changes in blood vessels.
5. Congestion and edema: particularly in the lungs, brain, and upper airways.
There should be signs of hypoxia (oxygen deprivation) in brain tissues. Also, a microscopic examination of brain slides may reveal swelling or changes indicative of anoxia or ischemia. And then there were the lung findings - signs of pulmonary edema (fluid in the lungs) as well as possible aspiration of blood or stomach contents, in cases where suffocation causes gagging or regurgitation. As Cooke had pointed out, Lalita had a full meal in her stomach. Surely, surely if you are being gagged with a plastic bag, you would be sick and bring up the contents of your stomach?
On the 10th February, I had LIA write a letter to the Attorney General, Toni Buti, explaining the problem with the coroner permitting the cremation Of Lalita Horsman.
Following earlier correspondence with the Coroner’s Court, I was advised that, as a matter of general practice, cremation is authorised only once the forensic pathologist has advised that all necessary testing and examinations have been completed, notwithstanding that final reports may issue later. I accept that explanation of general process.
However, having now reviewed primary laboratory records, sworn evidence, and the documented timeline in this matter, I am concerned that, in this case, that assurance may not have been factually sound.
The post-mortem examination was concluded on the night of 9 December 1999. Lalita Horsman was cremated on 14 December 1999, five days later. This interval is significant. It provided sufficient time for further laboratory testing to be undertaken, completed, or at minimum initiated, had it been regarded as necessary.
A Chemistry Centre (WA) report dated 14 December 1999 confirms that while blood and liver samples were analysed for common drugs, stomach contents were explicitly recorded as “Not Analysed”, despite having been submitted.
As you would appreciate, toxicological exclusion of drug overdose cannot be achieved without analysis of stomach contents, and visual inspection alone is not a substitute for laboratory testing. At the same time, the pathologist’s sworn evidence confirms that there was no anatomical or toxicological explanation for death, and that the later characterisation of the cause of death as “unascertainable (consistent with asphyxiation)” rested largely on contextual information rather than demonstrable pathology.
I am not seeking immediate action, nor making any allegation of bad faith. I am seeking guidance as to whether, and how, this apparent disconnect between assurance and record might be examined at an executive or institutional level, with a view to strengthening confidence in coronial and forensic processes. If you consider it useful, I remain willing to meet with you, or to brief a member of your office, to outline the evidentiary material and forensic concerns in a private and responsible setting.
I fully understand if that is not possible, and in that event I will continue to proceed carefully and independently. I would be grateful for any direction you are able to provide.
It would be so much easier if they would only look at my evidence and allow me to work with them for a better justice system.
Unfortunately, the moment they are officially aware of the problem, they can never use the excuse “we didn’t know anything about this.”


Comments